Colleen Grablick
Colleen Grablick
Months after the monkeypox – now called mpox – outbreak surged in the D.C. region, cases have continued to fall dramatically, which experts say underscores the efficacy of smart public health strategies, while also illuminating ongoing equity gaps.
“I think we have a case for public health, of how a community can respond to an outbreak, and in fact significantly reduce new infections and protect not only the LGBTQ community but the community in general, because we were able to contain the outbreak,” said Dr. Carlos Rodriguez-Diaz, an associate professor in the prevention and community health department at George Washington University’s Milken Institute School of Public Health.
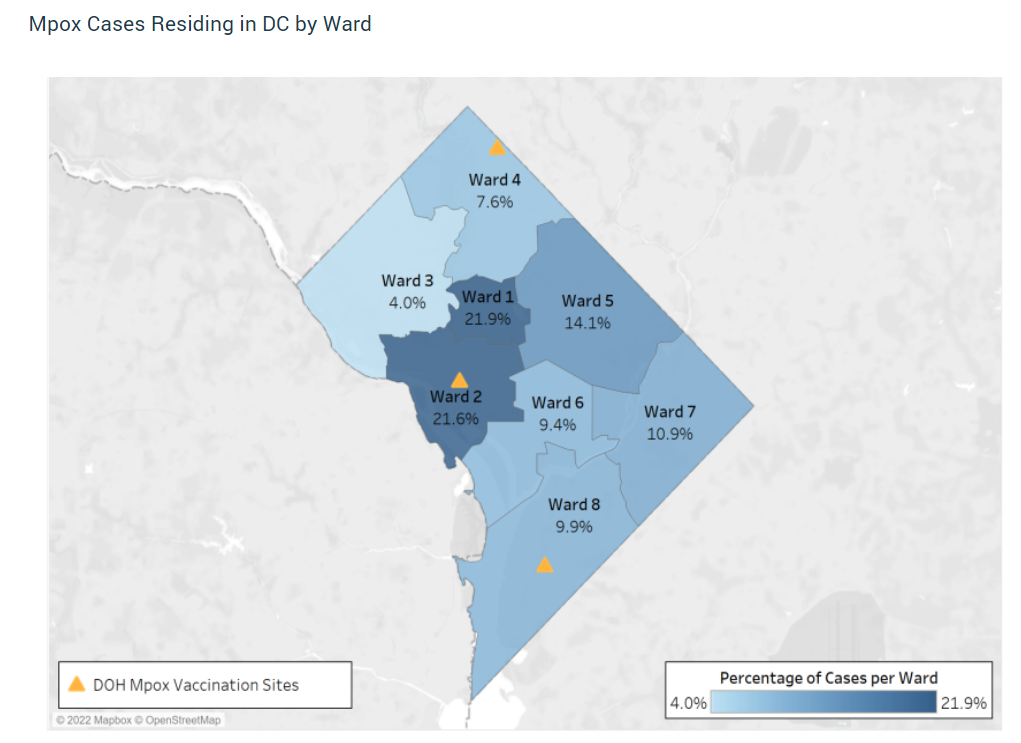
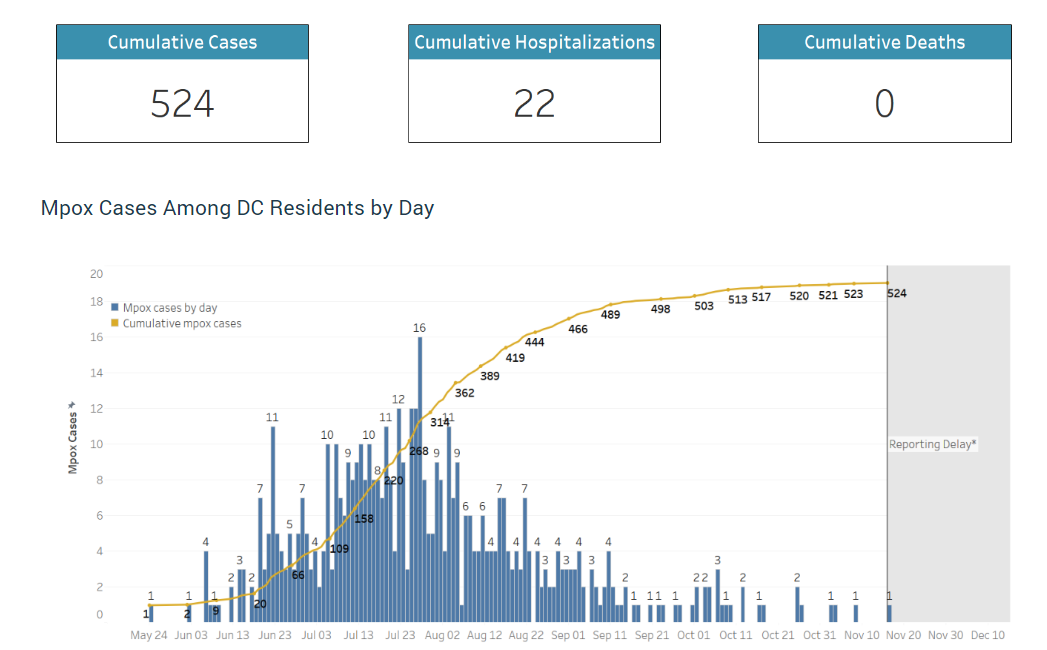
The District once had the highest number of mpox cases per capita in the U.S., but since mid-October the city has reported a rolling weekly average below 0.5, recording between 0 to 2 cases a day. Since the local outbreak began in early June 2022, the city has reported 524 cases, 22 hospitalizations, and no deaths, with the highest percentage of cases occurring in the city’s Wards 1 & 2.
The situation looks similar around the region. Cases fell in Virginia throughout September and October, with the commonwealth reporting a total of four cases in the last two weeks of November. A majority of Virginia’s 559 cases have been reported in the Northern region, with Fairfax County reporting the most infections of any county in the commonwealth at 90 cases. While cases have dropped off, Virginia reported its first death from the virus earlier this month, in the Eastern region. In Maryland, which has reported a total of 733 infections, 33% of cases have occurred in Baltimore City, while Prince George’s County accounts for 31%, and Montgomery County 12%. Three residents have died of the virus in the state.
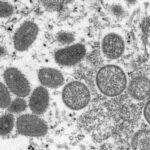
Mpox, a virus similar to smallpox that spreads predominantly through close contact with infectious rashes, scabs, or bodily fluids, typically causes flu-like symptoms similar to COVID-19. The sores caused by the virus can be incredibly painful, but the current outbreak of mpox has proved to have a relatively low death risk. Across the U.S., 20 individuals have died of the virus, according to the Centers for Disease Control and Prevention.
This fall’s plummeting case counts marked a sharp departure from the mpox landscape earlier this summer. Hamstrung by a bungled federal vaccine rollout and limited testing, local health officials walked a fine line as they tried to stretch a limited vaccine supply by prioritizing the most at-risk populations — while also trying to avoid stigmatizing the LGBTQ+ community, or replicating the equity failures of the COVID-19 vaccine rollout.
In the initial weeks of the outbreak, D.C. limited its vaccine availability based on certain criteria (gay, bisexual, and other men 18 and older who have sex with men and have had multiple recent partners, sex workers, as well as staff of establishments where sexual activities occurs.) But by mid-August, any resident with multiple recent partners could get a vaccine at one of the city’s weekly walk-up clinics or by booking an appointment online — regardless of their gender or sexuality.
Jason Cianciotto, the vice president of communications and policy at the Gay Men’s Health Crisis, says that while increasing availability of the vaccine played a big role in curbing the outbreak, community-based public health efforts that leveraged the networks and know-how of queer health organizations was also crucial. Similar to COVID-19 vaccination efforts, Cianciotto says it’s important for certain information to come from a trusted member of the community, rather than a government agency or health provider.
“Stigma and shame, homophobia, transphobia, all have an effect on where people choose to get health care, not just for HIV, but also for mpox,” he says, citing the success of efforts that utilized existing connections with groups already connected to at-risk communities.
For example, D.C. organizations like Us Helping Us, a health provider for gay and bisexual Black men and transgender women, and the local harm reduction agency HIPS, launched messaging campaigns to make clients aware of resources. They also hosted pop-up vaccine clinics. The city also worked with Whitman-Walker, a health provider focused on serving the LGBTQ+ population.
“We learned from fighting the HIV epidemic for 40 years that in order to effectively reach communities who are at higher risk – often because of mistrust with healthcare communities or because they come from racial and ethnic backgrounds where there are even higher rates of homophobia and transphobia – that having someone meet with a prospective client who represents the community they’re from goes a long way towards building that trust,” Cianciotto says.
While infection levels have significantly improved, disparities have also become clear.
“We are seeing, though, a disparity in terms of vaccine uptake,” says Rodriguez-Diaz of the Milken Institute. “Most of the vaccines have gone to white arms – and we are still seeing that the new infections are predominantly among men who have sex with men and who are also Black, Latino, or non-white men.”
In D.C., white residents make up 36% of cases, while Black residents make up 40%. But 54% of vaccinations have gone to white residents, per the city’s data, while 20% have gone to Black residents. This gap is larger nationwide, with white people accounting for more than 330,000 first doses, while Black people have received 80,000 and Latino people roughly 145,500. Meanwhile, white people in the U.S. account for 28% of cases to Black people’s 38%. Latino people account for 24%.
“Targeted communications strategies, equitable placement of vaccination services, and strategic community partnerships have all helped to limit the racial gaps between infections and vaccinations where disparities still exist,” a DC Health spokesperson said to DCist/WAMU in an email, when asked what the city is doing to address the equity gaps. “DC Health continues to address these disparities through its programming every day.”
Cianciotto says the numbers indicate that more can be done to reach those who haven’t yet received a vaccine, particularly those who may not feel comfortable sharing their information with a local health department due to medical racism or homophobia.
“The communities who are now at highest risk are also the ones who are least likely to feel comfortable accessing healthcare or accessing something that they think will be reported to the government,” he says. “It could cause a problem for them because they’re undocumented or a sex worker, so that’s why I think it’s important that public education and outreach continue.”
As advocates continue to stress the importance of outreach and messaging, the Biden administration is set to let the national public health emergency declared over the virus lapse on February 1, citing the low case counts of the past several months. (D.C., Maryland, and Virginia never declared city or statewide emergencies over the virus, although New York City and San Francisco did.)
It’s possible, Rodriguez-Diaz says, to reach “mpox zero,” or eradicate the virus. D.C. has been reporting zero-case days for months, but the trajectory of the virus is dependent on what happens in other parts of the U.S. and world. While all states with outbreaks have largely seen infections subside over the past several months, other countries still have a limited vaccine supply. Even if the virus seemingly dies out in D.C., a surge in other countries where there is ongoing vaccine disparity could lead to the same problem reappearing locally.
“I think it’s time that if we really want to eradicate and get to zero, we need to work with partners elsewhere, to make sure that we don’t create national disparities in terms of the outbreak,” he says. “So at the local level, we are very close to achieve zero new infections for sustained amount of time, but that would not be sustained if we do not control the outbreak elsewhere.”