Colleen Grablick
Colleen Grablick
More than a dozen residents, doctors, and public health professionals testified before the D.C. Council on Thursday, supporting a long-held demand that Mayor Muriel Bowser declare a public health emergency in response to the city’s worsening opioid crisis.
“We cannot continue on this path without a public health emergency,” said Ambrose Lane Jr, the chair of the Health Alliance Network, a group that advocates locally for health equity. Lane led a rally outside the Wilson Building earlier this spring, issuing the same plea. “We have an epidemic that does not seem to be abated, regardless of the action that’s been taken by DC Health or Behavioral Health.”
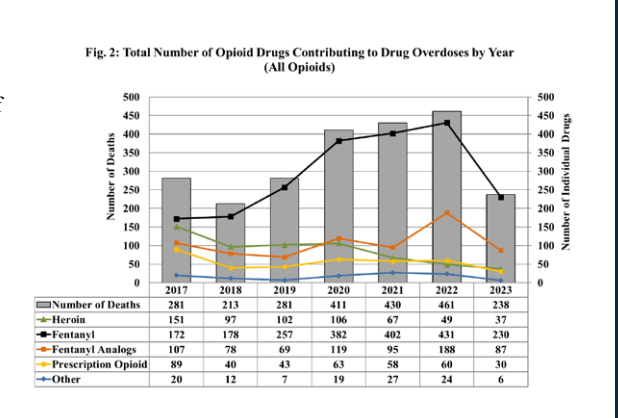
The urgent pleas for action — which have been ongoing for years — come as the city is on track to record its sixth consecutive year of record-high overdose fatalities. According to the Office of the Chief Medical Examiner, the opioid epidemic has killed 296 people through the end of July of this year, many of those people older Black men in wards 5,7, and 8. That’s a 17% increase from the same time in 2022, which saw a total of 461 deaths by year’s end, the deadliest year on record and more than double the number of homicides in the city. (The OCME only accounts for fatal overdoses — the number of total overdoses occurring in the city, some of which are reversed, is likely much higher.)
In mid-Sept., while the city’s fatal overdose rate continued to climb, all D.C. councilmembers circulated and signed a “sense of the council” (essentially a resolution expressing the council’s opinion) calling on the mayor to declare a public health emergency. Similar to what the city did at the onset of the COVID-19 pandemic, such a move would allow the city to access emergency resources, equipment, and federal funding, and facilitate greater coordination between city agencies. It would also, councilmembers wrote, bring more public awareness to the issue, opening avenues for education and intervention among young people. Neighboring Maryland and Virginia and the federal Department of Health and Human Services have all issued public health emergency declarations.
Over the course of the hearing, many who testified (including councilmembers) reiterated frequent critiques of the administration’s response to the crisis; most simply, that it’s woefully failing the city’s most vulnerable residents. While D.C. has made strides in expanding certain services (like increased distribution of the overdose-reversing drug Narcan), harm reduction advocates, doctors, and lawmakers said the city’s response is reactive, scattered across various programs, often rooted in criminalization, and falling far short of what’s needed.
“We have been extremely concerned with the mayor’s response to this crisis,” said Heidi Ellis, an organizer with Decrim Poverty D.C., a local coalition that advocates for the decriminalization of drugs and broader harm-reduction services. “Regardless of the overwhelming data, the countless testimonies from folks on the ground, and even urging from those in her administration, she continues to be inadequate in her response.”
A spokesperson for the mayor’s office did not offer comment on the hearing or the council’s proposed resolution. The spokesperson routed DCist/WAMU’s requests for comment to the interim deputy mayor for health and human services, Ciana Creighton. Creighton said the overdose increase rate year-over-year is not increasing, but “plateauing” — evidence that the city’s interventions are working.
It’s true that the city’s recent yearly increases in fatalities are not as drastic as the increase from 2018 – 2020 (overdose deaths increased from 213 in 2018 to a devastating 411 by 2020). However, the city is now regularly recording more than 400 deaths per year. From 2020 to 2021, deaths increased by 4.6%. In 2022, 461 people died, a 7.6% increase from the year prior. The rate of increase is not plateauing, but continuing to go up.
“We recognize the urgency in responding to the opioid epidemic, one that, while ever-changing, is not new. One death is a death too many,” Creighton said in a statement.
Director of the Department of Behavorial Health Barbara Bazron defended the city’s efforts to curb the crisis so far. She touted D.C.’s Narcan distribution, campaigns to destigmatize drug use, and the expansion of recovery housing, among other government services. But, as the chair of the council health committee, Christina Henderson pointed out in the hearing, Bazron failed to acknowledge whether the Bowser administration stands behind treating the crisis as a public health emergency.
“[Your testimony] was comprehensive in nature, yet didn’t necessarily answer the central question of whether or not the Bowser administration views the opioid crisis in the city right now as a public health emergency,” Henderson said. In response, Bazron said the administration is “certainly willing to have the discussion.”
Zachary Parker, the Ward 5 councilmember, pressed Bazron further to name the devastating numbers of fatalities as a crisis. Bazron failed to use the word, but said “one death is one too many.”
“It’s a little frustrating that this is the fourth or fifth hearing we’ve had [on this issue] and we can’t even just clearly say we have a crisis, one that is primarily impacting communities like mine,” Parker said. “I have no doubt that you [Dr. Bazron] are thinking about these things…I’m not persuaded that whoever is leading a broader central coordination across the executive team is thinking about that.”
Bazron and DBH are in the process of updating the city’s comprehensive opioid response plan, Live Long DC, and the city is set to open a new sobering center later this fall in Ward 6. (That sobering center was initially slated to open in the spring but has been repeatedly delayed. On Thursday morning, a spokesperson for DBH said they would be alerting DCist/WAMU of an opening date “soon,” but no date has been circulated yet.) The city is also fielding applications for a forthcoming 24/7 substance use and opioid use treatment center specifically for young people — a consistent demand from organizations like the Health Alliance Network.
Yet even the plans in place are not enough, those who testified on Thursday said, as they offered a bevy of different solutions and avenues for emergency dollars to be spent.
“All of those things are laudable,” Lane said of the city’s advancements to address the opioid epidemic thus far. “But they are not going to solve this crisis. We need leadership…the mayor needs to step up.”
Harm reduction advocates — including LJ Sislen, an outreach volunteer with HIPS DC, and Queen Adesuyi, formerly a policy manager at the Drug Policy Alliance — re-upped a call for the city to create two harm reduction centers, also known as overdose prevention centers. These are places where people can go to safely use drugs under medical supervision (in addition to accessing a wide variety of wrap-around services). Elsewhere across the globe, these centers play a significant role in overdose prevention strategies but have been slow to take off (or outright banned) in state and local U.S. governments. Two such centers currently exist in New York City, run by the group OnPointNYC; in their first year of operation, OnPoint stopped hundreds of overdoses while recording zero deaths.
Certain federal statutes could stand in the way of D.C. opening its own overdose prevention centers, and opioids remain criminalized in the city. Just this week, Bowser introduced legislation that would re-instate “drug-free zones,” an advent of the War on Drugs that the D.C. Council previously voted out in 2014. The proposal would allow the police to prevent individuals from gathering in certain areas for up to five days, and apprehend anyone they suspect of participating in drug activity. (Even something like track marks on an individual would be, under the law, justification for the police to stop them.) Sislen and Adesuyi both pushed back against criminalization policies, which research has shown does not curb use or prevent death.
“Punishment and stigma don’t work, but investing in health, housing, and other social services does,” Sislen said. “The last place a person with a substance use disorder should be at is a cell…the trauma continues to negatively impact people when they return home, whether that be a higher likelihood of overdosing, getting access to safe housing or social services; it also increases recidivism rates, and that just proves the inefficiency of jails and prisons’ ability to rehabilitate drug use.”
Several behavioral health and medical professionals also testified to the urgency of the problem on Thursday and to the city’s failing, fragmented net of social services that is fueling the crisis.
“In my experience, I’ve never seen a situation as bad as it is right now,” said Dr. Edwin Chapman, a physician who has been treating D.C. residents with opioid use problems for decades.
Chapman has been on the frontlines of medically-assisted treatment advocacy in D.C., or the practice in which people dependent on opioids are provided with medication like buprenorphine. He called on the city to improve coordination between mental health supports, housing providers, and medical care, so residents aren’t left on their own trying to manage multiple, often complicated, government services.
“If you don’t have the leadership from the government, we will continue to have a fragmented approach where people operate in silos,” Chapman said.
Dr. John Dombrowksi, an anesthesiologist at the Washington Pain Center, said the city’s current infrastructure for treating opioid use — particularly for individuals with long-term use, co-occurring mental health disorders, or co-occurring physical conditions — is held together with “gum and duct tape.”
“We’ve got a lot of resources, but there’s no coordination of care,” he said. “That’s the biggest problem I see…it’s shampoo, it’s wash, rinse, repeat, and hoping for different outcomes.”
In addition to the additional funding that could be made available under a public health emergency, D.C. is also set to receive tens of millions of dollars for opioid solutions over the coming years as a part of settlements with major drugstores and pharmaceutical manufacturers. Currently, the city’s fund has some $14 million dollars in it — but that money sat stale for months due to bureaucratic lags. Earlier this year, the D.C. Council passed legislation creating a new office for opioid abatement and establishing a commission to oversee the dispersal of the settlement funds. None of those settlement dollars could be touched until the council and the mayor respectively appointed the 21-person commission. Originally, the group was supposed to have formed and met by the end of the summer — but full appointments weren’t finalized until mid-October. The commission, which consists of several government officials and a handful of medical and behavioral health specialists (including Chapman) just had its first meeting on Wednesday.
Larry Bing, a peer mentor who works in Dr. Chapman’s office and also sits on the commission, said after their first meeting on Wednesday, he did feel slightly disappointed in the apparatus set up to solve the issue. But speaking at the hearing, he said those working to reduce deaths can’t let that disappointment make them lose sight of the goal.
“I still want the mayor to call it what is, but even if she doesn’t I’m not gonna stop doing what it is we do, helping out clients,” Bing said. ” I don’t want us to lose sight of that. We need to continue our platform, make sure the work we’re doing gets done.”
This story has been updated with a statement from the interim deputy mayor for health and human services.