 Margaret Barthel
Margaret Barthel
Five months in, a program in Alexandria that pairs first responders with mental health clinicians when responding to behavioral health-related emergency calls is meeting with some success and some challenges. An assessment produced by the OMNI Institute, an independent consulting nonprofit, will be reviewed by the City Council on Tuesday evening.
The Alexandria Co-Response program (ACORP), launched in September 2021, partners a police officer with a licensed mental health worker to respond to 911 calls. Reducing or removing police entirely from responding to calls with a mental health component has gained traction regionally and nationally — particularly in the wake of police shootings of people in mental health distress — as an approach that could cut down on arrests of people who need behavioral health care, not jail.
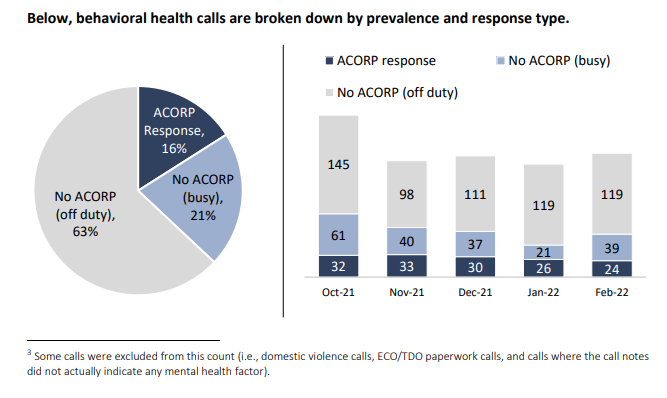
From Oct. 2021 to Feb. 2022, ACORP — which is currently only two people, a clinician and a police officer — responded to a total of 145 calls to 911, more than half for unusual behavior or threats of self-harm. Of the calls that the study determined could have resulted in an arrest, 71% diverted people towards other services.
The pair were able to resolve the problem in person on the scene in a little less than half of all the calls (45%). In other cases, they referred people to community services that could help them (20%) or were able to transport someone voluntarily to a hospital, shelter, or other service for support.
Just 13% of the calls ended in an involuntary transport to the hospital.
While ACORP only responded to about 15% of the 958 calls that had a behavioral health element, an additional 65% of those calls were responded to by a police officer trained in crisis intervention and de-escalation tactics, a training hundreds of Alexandria officers have undergone since 2009.
Comparing between the three different possible responses to a behavioral health emergency in Alexandria — ACORP, crisis-trained officers, or officers who have no behavioral health-specific training — the initial data suggests that ACORP was significantly more effective at resolving problems on-scene, and somewhat more likely to refer people in crisis to community services. They were significantly less likely to transport people to hospitals or shelters, especially on a non-voluntary basis.
ACORP responders are serving people with a similar demographic profile to clients of the city’s Community Services Board, which provides support for people with mental health needs, developmental disabilities, and substance use disorder.
In addition to the data, the report describes several response calls led by ACORP where the group appears to have made a material difference in the outcome of the incident. In one case, for example, ACORP members successfully de-escalated a situation involving a person who had been cutting himself with a knife, the presence of which had caused many police officers to rush to the scene and surround the man.
“The individual shared that he did not trust the police due to previous negative encounters and threatened to harm anyone coming close to him physically,” the report documents.
The man in distress eventually agreed to talk with the ACORP clinician alone, with the partner ACORP officer still in the room. The ACORP team asked the other officers to leave the room quietly, and from there was able to get the man to give up the knife and go with them voluntarily to the hospital for further care.
While the initial data results from ACORP are encouraging, the report suggests there are some challenges ahead. The areas of improvement it suggests range widely, including creating better training for 911 call screeners about which calls ACORP should be assigned to and figuring out how to bridge the gap between law enforcement and mental health clinician cultures. That could also include sorting out how to get multiple different data systems to work together to track the group’s outcomes without manual entry.
The study acknowledges that health and public safety administrators in Alexandria are building the plane while they’re flying it.
“Prior to the launch of ACORP, the team consulted with several nearby jurisdictions to better understand the co-response model,” the report says. “Much of what they learned from these consultations was that most co-response programs operate in a ‘learn as you go’ manner, in that there is not a prominent training model in the field to guide law enforcement or clinicians as to how to engage in this partnership successfully.”
Another major challenge is staffing for the unit.
“Not only are there behavioral health calls for service that are not receiving an ACORP response, but the ACORP team is limited in terms of the ability to take time off as needed for individual well-being and program sustainability,” the report says.
Alexandria’s 2023 budget, recently passed by the City Council, includes funding for two more ACORP teams.
The fledgling Alexandria program represents at least one step towards fulfilling a soon-to-be state-mandated requirement to tailor law enforcement emergency responses to behavioral health situations.
In 2020, the Virginia General Assembly passed the Marcus-David Peters Act, named for a Black teacher shot and killed by Richmond police in 2018 while he was having a mental health crisis. The law outlines the creation of a so-called Marcus Alert system, a model that filters 911 calls involving behavioral health issues through regional call centers, in an attempt to tailor law enforcement responses to behavioral health needs on the scene.
The legislation requires localities to develop methods for responding to those behavioral health needs — perhaps through a “community care team,” which the law defines as a “team of mental health service providers, and may include registered peer recovery specialists and law-enforcement officers as a team, with the mental health service providers leading such team, to help stabilize individuals in crisis situations,” much like ACORP.
Five localities around the commonwealth, including Prince William County, already have Marcus Alert systems in place. The rest — including Alexandria — have until July 2026 to implement the system and create community care teams.
This story has been updated with information about Alexandria’s 2023 budget.



